Metabolic Syndrome
Metabolic syndrome is a cluster of conditions that occur together and increase the risk of heart disease, stroke, and type 2 diabetes. These conditions include:
- High blood pressure: Blood pressure of 130/85 mm Hg or higher. Hypertension.
- High blood sugar: Fasting blood sugar of 100-125 mg/dL (impaired fasting glucose) or diagnosed type 2 diabetes.
-
Obesity and excess fat around the waist: Body mass index (BMI) of 30 or higher. Excess fat in the stomach area (waist measurement of 40 inches or more for men, 35 inches or more for women).
- High triglycerides: 150 mg/dL or higher. Triglycerides are a type of fat found in the blood.
- Low HDL (good) cholesterol: 40 mg/dL or less for men, 50 mg/dL or less for women.
Having three or more of these conditions increases your risk of metabolic syndrome. The underlying causes of metabolic syndrome include insulin resistance, obesity, physical inactivity, and
genetic factors.
The diagnosis and treatment typically includes:
- Lifestyle changes: Losing weight, eating healthy, reducing calories and carbs, exercising regularly. These can help reverse the syndrome.
- Medications: Such as statins for high cholesterol, antihypertensives for high blood pressure, metformin for high blood sugar.
- Regular screenings: To monitor blood pressure, cholesterol, blood sugar, and other health indicators. Catching and managing the conditions early is important.
The key goals are to prevent or delay the development of heart disease and diabetes, while improving health and quality of life. Managing metabolic syndrome requires commitment to long-term
lifestyle changes and close monitoring of health.
Topic Highlights:-
- Metabolic syndrome is defined as a clustering of major cardiovascular risk factors along with abdominal obesity.
- Risk factors include high blood pressure, obesity, low HDL cholesterol, raised triglycerides, high cholesterol, and glucose intolerance.
- The root cause of metabolic syndrome is thought to be insulin resistance.
-
This presentation provides information on metabolic syndrome and its constituent conditions - diabetes, insulin resistance, hypertension and dyslipidemia, with a note on the risk factors and
management of the condition.
Transcript:-
Metabolic syndrome defines a clustering of major cardiovascular risk factors, in association with (central)obesity and excess weight, which includes at least two of the following four risk factors
i.e.; raised blood pressure, low HDL cholesterol, raised triglycerides and glucose intolerance
Millions of people have metabolic syndrome. It affects approximately 20% of adults in developed countries and 80% of people with type 2 diabetes. While the syndrome itself may not affect quality of
life, if left unchecked, it is associated with increased risk of type 2 diabetes by 9 to 30 times and heart disease by two to four times. It is very strongly linked with central obesity and the
worldwide rise in obesity is predicted to lead to a rise in the number of people with metabolic syndrome. It can affect about 5% of those with normal weight; 22% of those who are overweight and nearly
60% of the obese. The risk of developing metabolic syndrome increases by up to 45% in those who continue to gain five pounds or more weight per year.
The root cause of the metabolic syndrome is thought to be insulin resistance. Obesity and abdominal obesity in particular, lead to insulin resistance, that starts a process that includes accelerated
atherogenesis and often culminates in diabetes, heart and vascular diseases and stroke.
Metabolic syndrome was first described by Reaven and colleagues in 1988 as a link between insulin resistance and hypertension, type 2 diabetes, dyslipidemia and other metabolic abnormalities that
increased an individual’s risk of developing atherosclerotic cardiovascular diseases. The components of metabolic syndrome include obesity with an increase in waist measurement; hypertension;
dyslipidemia and glucose intolerance.
Other components may include microalbuminuria; evidence of a prothrombotic state with elevated blood fibrinogen and plasminogen activator inhibitor–1 level; and increased inflammatory markers such as
raised blood CRP.
There are several definitions of metabolic syndrome as defined by a variety of international bodies. However, the ones most often referred to are the definitions and guidelines framed by the World
Health Organization (WHO), the National Cholesterol Education Project Adult Treatment Panel (NCEP-ATP III); and the International Diabetes Federation(IDF).
According to these definitions, the numerical values assigned to the constituent conditions of metabolic syndrome are:
Hypertension: Patients who are currently on antihypertensive medications; or those whose systolic blood pressure is greater than 130 mmHg or those whose diastolic blood pressure is greater than 85
mmHg.
Dyslipidaemia: Patients who have blood triglyceride levels higher than 1.7mmol/L or 150 mg/dL and/or patients whose blood HDL levels are less than 0.9mmol/L or 35 mg/dL if males and 1.0mmol/L or
40mg/dL if female.
Obesity: Patients with a BMI of more than 30 kg/m2 and/or whose waist circumference is more than 40 inches, if male and more than 35 inches, if female; or whose waist to hip ratio is more than 0.9, if
male and more than 0.85, if female. Waist circumference less than or equal 94cm for Europid men and less than or equal 80cm for Europid women is defined as central obesity.
Glucose: Patients with Type 2 diabetes or with impaired glucose tolerance; or patients whose fasting blood glucose is in excess of 5.6mmol/L or 100mg/ dL.
Microalbuminuria: Patients with overnight urinary albumin excretion rate of more than 20 mcg/min or 30 mg/g Cr.
According to the WHO definition, for a confirmed diagnosis of metabolic syndrome, the patient should have Type 2 diabetes or impaired glucose tolerance plus any two of the other constituent
conditions. If glucose tolerance is normal then the patient needs to exhibit at least three of the other constituent conditions.
According to the NCEP-ATP III, having any three out of the five conditions (expanded waist, raised triglyerides, low HDL cholesterol, raised blood pressure and glucose intolerance), leads to a
diagnosis of metabolic syndrome.
According to the IDF, patients with central obesity and any two of the other four conditions qualify for a diagnosis of metabolic syndrome.
The major risk factors for developing metabolic syndrome are obesity and abdominal or central obesity combined with a sedentary lifestyle. There are also likely to be genetic susceptibility factors
and other environmental factors which include smoking, alcohol consumption, menopause, high carbohydrate diet, age and ethnicity.
Metabolic syndrome shows a highly age-dependent prevalence. It’s less common below 30 years and more common in middle age and beyond; however, the incidence of metabolic syndrome in children and
adolescents is on the rise due to the increasing incidence of overweight and obese children. The prevalence of metabolic syndrome in certain population groups is particularly high. These include South
Asians where there is associated evidence of increased rates of abdominal/central obesity and in Mexican and Black Americans. Low birth weight has been linked to increased risk of obesity and diabetes
in adulthood and consequently to increased risk of metabolic syndrome.
Insulin is a hormone produced by the beta cells of the pancreas and released into the bloodstream where it’s taken to the various tissues within the body where it produces its biologic effects. It
plays an important role in the metabolism of carbohydrate, lipids and proteins, and helps regulate cell growth. Insulin resistance is a condition in which the normal quantities of insulin fail to
produce the required biologic effects. This means that in a person with type 2 diabetes and insulin resistance, many units of insulin per day may be required to produce glycemic control.
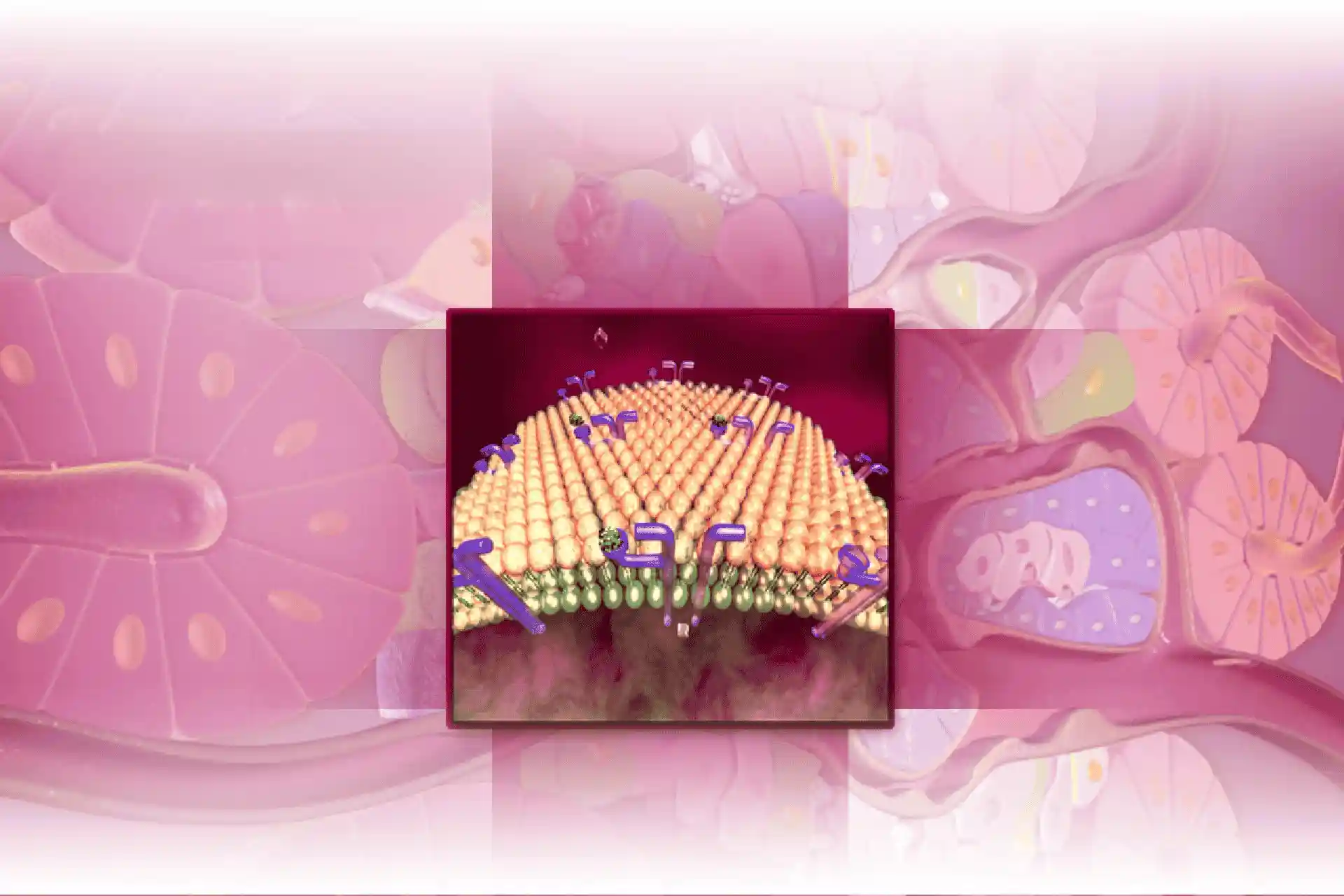
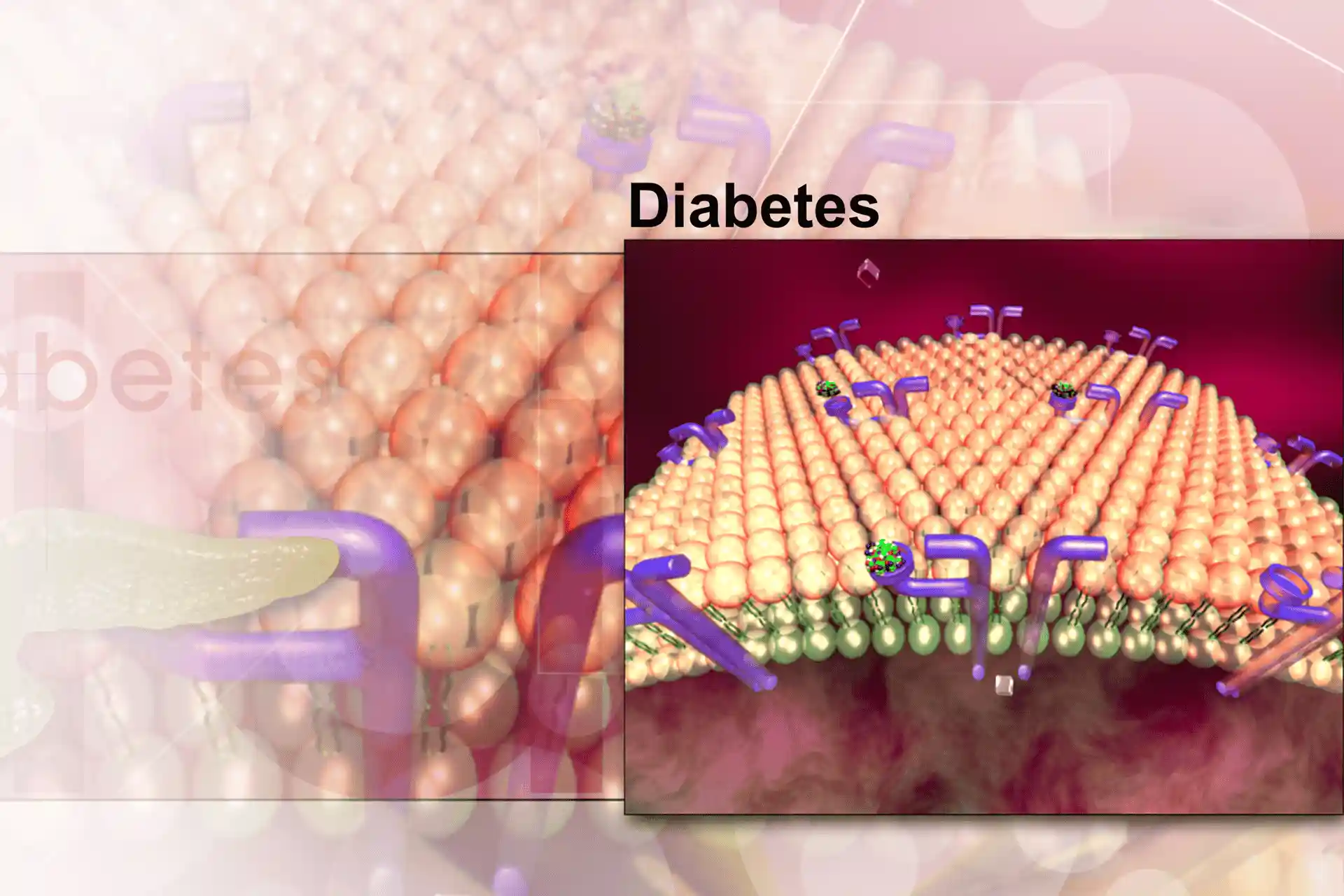
Insulin produces its biologic effects by binding to insulin receptors and insulin-like growth factor 1 (IGF-1) receptors present on cell surfaces of target tissues like skeletal muscle, liver, kidneys
and adipose tissue. The insulin receptor is a heterotetrimeric molecule that has two beta chains, which extend extracellularly and two ß chains that are present across the cell membrane. These chains
are linked by disulfide bonds. The cytosolic end of each ß chain carries tyrosine kinase activity.
When an insulin molecule binds to the trough created by the two alpha chains, the insulin receptors undergo a conformational change such that the two ß chains come closer to each other and cause
transphosphorylation of their tyrosine residues. This autophosphorylated insulin receptor kinase gets rapidly absorbed into endosomes. The endosomal system then regulates insulin-signaling pathways.
Postreceptor signaling pathways within the target cells bring about the action of insulin.
While many factors can affect the concentration of insulin receptors and the affinity of insulin for its receptors, insulin resistance usually results from defects in the target cells, autoantibodies
to insulin and accelerated insulin degradation. The pathophysiology of insulin resistance is based at two levels: the effect that insulin has on the metabolic pathways in the body and the cellular
mechanisms involved in insulin utilization.
Abdominal obesity is strongly associated with insulin resistance. Central or abdominal fat is more metabolically active than peripheral fat. The rates of fat storage and fat release are greater in
central fat deposits than in peripheral fat collections. The link between central obesity and insulin resistance arises from a combination of increased production of chemicals (adipokines) produced
from fat cells – these include increased leptin and TNF-alpha and reduced adiponectin. This imbalance leads to increased atherogenesis. In addition, excessive free fatty acids are transported to the
liver due to a higher rate of lipolysis in abdominal adipocytes.
Insulin resistance develops due to the reduced peripheral insulin sensitivity caused by adipokine imbalance and the free fatty acid induced reduction in peripheral insulin sensitivity and reduction in
hepatic insulin uptake, degradation and sensitivity. There is also an increase in the production of the enzyme 11-beta-hydroxysteroid dehydrogenase type-1 in individuals with excessive abdominal fat.
This enzyme converts inactive cortisone to active cortisol, which encourages visceral fatty deposits and insulin resistance.
Most insulin resistance is manifested at a cellular level and away from the point where insulin interacts with its receptors. Intracellular signaling pathways that lead to insulin action are most
significant in development of insulin resistance.
The two major pathways activated by insulin binding to its receptor are the phosphatidylinositol-3'-kinase or PI3K pathway and the mitogenic or mitogen-activated protein or MAP kinase pathway. The
clinical manifestations of insulin resistance will depend on which one of the postreceptor signaling pathways has been disrupted because while the PI3K pathway is important for bringing about the
metabolic effects of insulin, cell growth and proliferation and procoagulant effects are associated with the MAP kinase pathway.
It has been confirmed in several prospective epidemiological studies across a variety of population groups that insulin resistance is an important precursor in the development of Type 2 diabetes. Type
2 diabetes begins with peripheral insulin resistance and travels across a continuum of worsening insulin action and may end up with a partial failure of the insulin secretory process. For most
patients, development of type 2 diabetes results from a combination of insulin resistance and impaired pancreatic beta-cell secretory capacity with progressive deterioration of beta-cell function over
time.
Insulin regulates muscle glucose uptake and limits liver production of glucose by gluconeogenesis. By limiting gluconeogenesis in the liver, and encouraging cellular uptake of glucose in skeletal
muscle cells insulin controls the amount of glucose in blood.
Insulin resistance can occur at three main sites: the liver, muscle and adipocytes. Peripheral insulin resistance involves defects in the postreceptor signaling pathways that prevent glucose uptake by
the muscle cells. This type of peripheral insulin resistance can occur in persons of normal body weight as well as the obese.
In persons with visceral adiposity, the adipocytes are resistant to the antilipolytic effect of insulin and hence release excessive amounts of free fatty acids which find their way to the liver
through the portal circulation. These free fatty acids in the liver increase gluconeogenesis and result in increased blood glucose. Increased gluconeogenesis combined with low peripheral glucose
uptake results in high blood glucose levels, also known as hyperglycemia. Hyperglycemia signals the pancreas to produce more insulin.
Besides this, high levels of circulating free fatty acids slow down the breakdown of insulin in the liver and further contribute to high blood insulin levels. Thus hyperinsulinemia occurs along with
hyperglycemia. This excessive basal glucose production in presence of fasting hyperinsulinemia is a characteristic early feature of type 2 diabetes, but progresses over time to reduced insulin
secretion.
Dyslipidemia and hypertension are often found in individuals with insulin resistance. The compensatory hyperinsulinemia seen in insulin resistant individuals leads to an increase in the synthesis of
very low-density lipoprotein or VLDL in the liver. VLDL is converted into triglycerides and LDL and is released into the circulation. In peripheral tissues, insulin resistance results in the inability
of insulin to act on lipoprotein lipase, which is instrumental in the breakdown of triglycerides and LDL in tissues. These effects lead to elevation in plasma triglycerides and LDL cholesterol levels.
Insulin resistance also results in enhanced rate of synthesis of HDL; however, it seems to increase the rate of apolipoprotein A1/HDL cholesterol degradation even more, such that plasma HDL levels
reduce.
There is much clinical evidence that insulin resistance, specifically a disruption of the insulin-mediated glucose uptake, and the consequent hyperinsulinemia are common in hypertensive patients,
although not all hypertensive patients are insulin resistant.
Insulin resistant individuals are more likely to develop hypertension than those who are insulin sensitive. Further, the fact that insulin resistance often precedes the development of essential
hypertension has been proven in several prospective studies.
Insulin resistance results in disruption of the complex genetic, physiological and biochemical control systems that help maintain cardiovascular homeostasis and hence a predisposition to hypertension.
Insulin resistance causes chronic sodium retention and sodium sensitivity in the kidneys and increases excretion of water. Insulin resistance enhances the activity of the sympathetic nervous system
and stimulates growth of the vascular smooth muscle. All these changes contribute to elevating blood pressure.
Apart from dyslipidemia and hypertension, insulin resistance puts into motion a number of other mechanisms that lead to arthrogenesis and consequent atherosclerotic events. Insulin resistance results
in a chronic inflammatory state that is evidenced by increased C-reactive protein (CRP) in blood, which leads to a reduction in nitric oxide levels. Nitric Oxide or NO is essential for maintaining the
vascular tone of blood vessel walls and it plays an important role in dilating blood vessels and preventing damage to the endothelium during increased blood pressure or flow. Increased TNF- alpha
levels in the blood of individuals with central adiposity increases the ability of LDL cholesterol to bind to blood vessel walls, which is the first step toward the formation of atherosclerotic
plaques.
Abdominal adipocytes also secrete an adipocytokine that promotes thrombosis, called plasminogen activator inhibitor-1 or PAI-1. PAI-1 inhibits normal fibrinolysis and elevated plasma PAI-1 levels lead
to formation of new clots or augmentation of existing clots. In addition to these effects, visceral adipocytes produce less adiponectin which is a protective protein secreted by subcutaneous
adipocytes. Hence insulin resistant and viscerally obese individuals are deprived of the protective effects of adiponectin, which include increasing insulin sensitivity, protection of vascular
endothelium and reduction in circulating free fatty acids as well as increased clearance of triglycerides.
Dyslipidemia or high plasma triglycerides and low HDL levels, elevated blood pressure and damage to the vascular endothelium begin the process of arthrogenesis that culminate in atherosclerotic
diseases in individuals with insulin resistance.
Patients with metabolic syndrome have an increased risk of cardiovascular events and mortality so the main aim of management is to reduce that risk. This has led to a focus on lifestyle measures
including attention to diet, reduction of weight, increased physical activity and not smoking.
Initially the pharmacotherapeutic focus was on single risk factor intervention but this has now been replaced by multiple risk factor intervention using combinations of antihypertensives, low dose
aspirin (once blood pressure has been controlled), statins and antihyperglycemic agents (in cases with diabetes). There has also been interest in more directly targeting the underlying insulin
resistance through both lifestyle intervention and the use of drugs such as rimonabant, the first endocannabinoid-1 receptor blocker. The latter has a central appetite suppressant effect but also
peripheral effects including effects on fat at least partially correcting adipokine imbalance, with improvements in HDL, triglycerides and glycemic control. This drug is presently the subject of long
term trials of cardiovascular risk reduction and there is no doubt other drugs specifically targeting insulin resistance will be developed in the future.
For the present, lifestyle and multiple cardiovascular risk factor intervention remain the most important aspects of management of this increasingly prevalent condition.