Glaucoma
Glaucoma is a group of eye conditions that damage the optic nerve, which is crucial for good vision. This damage is often caused by an abnormally high pressure in your eye. Glaucoma is one of the
leading causes of blindness for people over the age of 60. Early diagnosis and treatment can help prevent vision loss.
Types of Glaucoma
There are several types of glaucoma, but the two main types are:
-
Open-angle glaucoma: This is the most common form of glaucoma, accounting for about 90% of cases. It occurs when the eye's drainage canals become clogged over time, causing an
increase in intraocular pressure (IOP).
-
Angle-closure glaucoma: This type of glaucoma, also known as closed-angle glaucoma or narrow-angle glaucoma, occurs when the drainage angle between the iris and cornea is too
narrow, resulting in a sudden increase in IOP. This can be an acute or chronic condition.
Other less common types of glaucoma include:
- Normal-tension glaucoma
- Congenital glaucoma
- Secondary glaucoma
- Pigmentary glaucoma
Causes
The exact cause of glaucoma is not fully understood, but it is believed to be related to the following factors:
-
Increased intraocular pressure (IOP): Elevated IOP is a significant risk factor for developing glaucoma. It occurs when the fluid known as aqueous humor builds up in the eye
due to an imbalance in production and drainage.
- Age: The risk of developing glaucoma increases with age, particularly after the age of 60.
- Genetics: There is a strong hereditary component to glaucoma, so having a family history of the condition increases your risk.
- Ethnicity: People of African, Asian, and Hispanic descent have a higher risk of developing glaucoma.
- Medical conditions: Diabetes, hypertension, and heart disease can increase the risk of glaucoma.
Symptoms
In its early stages, glaucoma often has no noticeable symptoms. However, as the disease progresses, symptoms may include:
- Gradual loss of peripheral (side) vision
- Blurred or distorted vision
- Eye pain or headache
- Halos around lights
- Nausea and vomiting (in acute angle-closure glaucoma)
- Redness in the eye
Diagnosis
A comprehensive eye exam is necessary to diagnose glaucoma. Tests may include:
- Tonometry: Measures the pressure inside the eye (IOP)
- Ophthalmoscopy: Examines the optic nerve for damage
- Perimetry: Assesses the field of vision
- Gonioscopy: Evaluates the drainage angle
- Pachymetry: Measures corneal thickness
Treatment
While there is no cure for glaucoma, early treatment can help slow the progression of the disease and prevent vision loss. Treatment options include:
- Eye drops: Prescription eye drops can lower IOP by either reducing fluid production or improving drainage.
- Oral medications: In some cases, oral medications may be prescribed to lower IOP.
- Laser therapy: Laser procedures can help improve drainage in open-angle glaucoma or open the drainage angle in angle-closure glaucoma.
- Surgery: Traditional surgeries, such as trabeculectomy, can create a new drainage pathway for fluid to exit the eye, lowering IOP.
It is essential to follow your eye care professional's recommendations for monitoring and treating glaucoma to minimize the risk of vision loss. Regular eye exams are crucial, especially for those
at a higher risk of developing the condition.
Topic Highlights:-
- Glaucoma is a group of eye diseases and the leading cause of blindness which occurs due to build up of intraocular pressure.
- The different types of glaucoma include primary open-angle, angle-closure, pigmentary, primary congenital, and secondary glaucoma.
- This animation describes the optical system, the various causes that lead to glaucoma, the animation highlights, the diagnostic methods, and treatment options available.
Transcript:-
Glaucoma, a group of eye diseases, is the leading cause of blindness in the world. This group of diseases often displays no symptoms at the outset. A gradual loss of vision develops that can severely
affect the quality of life of the patient. While glaucoma is most prevalent after the age of 60, certain populations such as African-Americans, Asians and particularly the Japanese are found to be
more prone to glaucoma beginning at the age of 40.
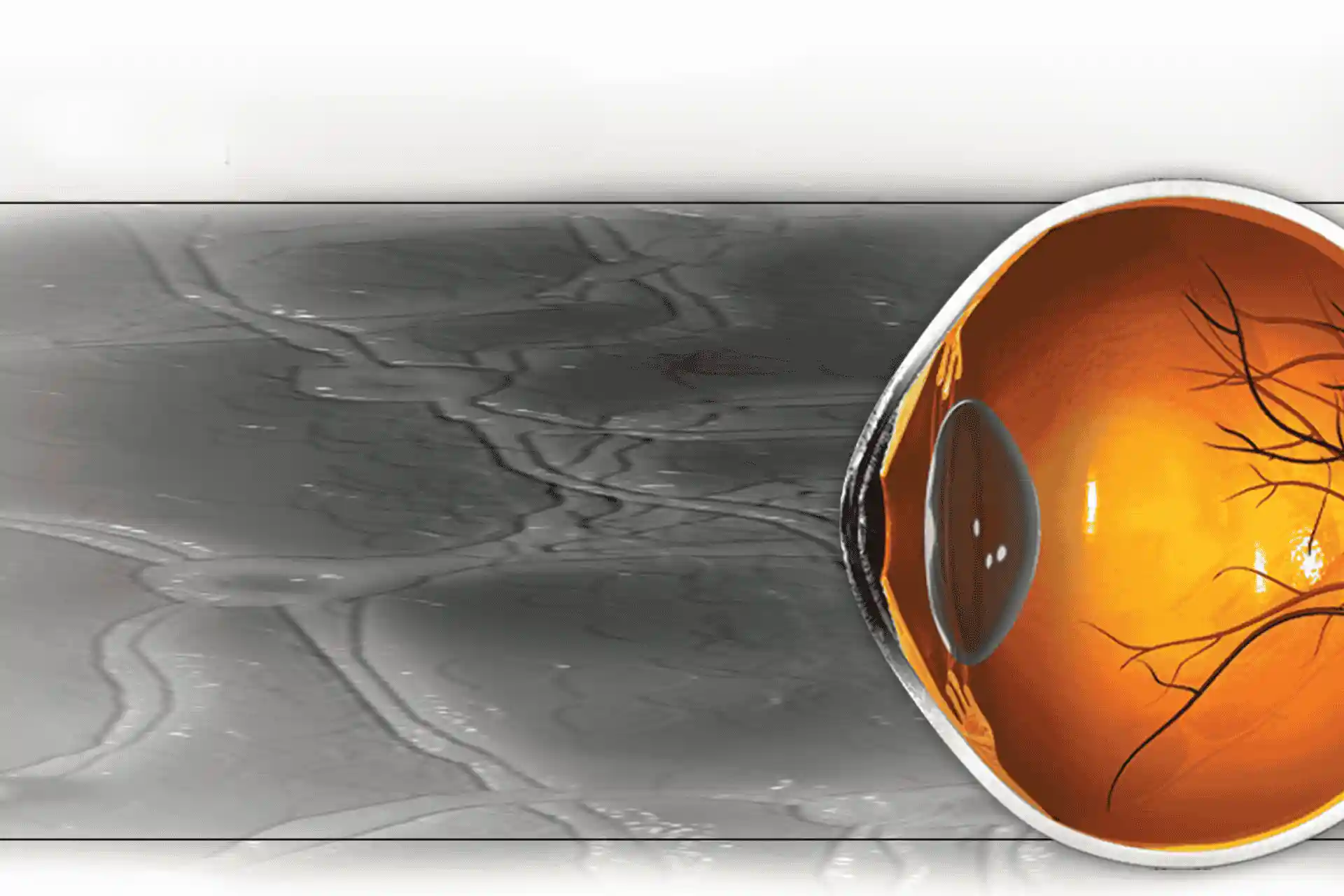
The eye's optical system consists of several structures in and around the eyeball. Light rays reflected from an object are bent, refracted and focused by the cornea, lens, and vitreous humor to focus
the rays onto the retina to form an image.
The cornea is the outermost covering of the eye behind which lies the aqueous humor, which is a fluid-filled chamber. Both the iris (the central part of the eye that controls the amount of light
entering the eye) and the convex lens (a flexible disc that helps focus rays of light onto the retina) lie behind the aqueous humor. The ciliary body is a group of muscles attached to the iris that
control changes in the aperture of the iris or the pupil as well as the lens shape for light focusing.
The anterior hyaloid membrane separates the lens and iris from the vitreous humor, a posterior fluid-filled chamber. The retina, which forms the posterior wall of this chamber, contains photosensitive
rod and cone cells, which generate nerve impulses when light falls on them. The choroid layer that lies behind the retina absorbs unused radiation. The optic nerve is a thick bundle consisting of
millions of nerve fibers that leave the eye from a blind spot on the retina called the papilla. Nerve impulses generated by the rods and cones in the retina are carried from here to the brain where
the image is perceived.
The aqueous humor nourishes the lens and the cells of the cornea and maintains pressure, which allows the cornea to maintain its convex shape which is necessary for good vision. The pressure inside
the eye (also known as intraocular pressure) is constantly maintained by the drainage of excess fluid out of the aqueous humor. The quantity of aqueous humor is carefully controlled and its fluid
constantly renewed and drained out through a sieve-like system called the trabecular meshwork. It is located around the base of the cornea near the ciliary body at the point where the cornea meets the
iris. The excess drained fluid enters the bloodstream through a duct called the Schlemm’s canal.
When the trabecular meshwork gets clogged and excess fluid cannot be drained, or when production of aqueous humor is in excess, the intraocular pressure builds up, damaging the optic nerve. This leads
to a group of diseases that are collectively called glaucoma.
The most common form of glaucoma is the primary open-angle glaucoma caused by inadequate drainage of the aqueous humor. It is called open-angle glaucoma because even though the trabecular meshwork
remains unclogged or open, the fluid drainage is reduced. With no visible obstruction detected, an increased resistance to the flow of eye fluid through the drainage system at a microscopic level
raises the pressure. Optic nerve damage and vision loss follows gradually and painlessly. The disease displays no symptoms until the increasing intraocular pressure affects the peripheral or side
vision. If left untreated, this could result in total loss of vision.
Angle-closure-glaucoma results when the drainage angle of the eye narrows due to a visible obstruction and the drainage system becomes completely blocked by tissue inside the eye, causing dangerously
high eye pressure. This emergency situation needs immediate medical attention to avoid total loss of vision. This type of glaucoma is often accompanied by severe symptoms that facilitate a quick
diagnosis. Severe eye pain, blurred vision, haloes around lights, headaches, dilated pupils, redness of the eyes, nausea and vomiting are some of the symptoms of acute closed-angle glaucoma.
Pigmentary glaucoma or pigment dispersion syndrome is an under-diagnosed type of inherited open-angle glaucoma affecting people in their twenties and thirties. It typically affects nearsighted
individuals, making it particularly dangerous to a lifetime of normal vision. This disorder is characterized by disruption of the iris pigment epithelium and pigment granule accumulation in the
trabecular meshwork which results in a blockage. Symptoms are not evident in this form of glaucoma.
Primary congenital glaucoma is present at birth due to a developmental abnormality that affects the trabecular meshwork. Glaucoma in infants is a rare condition and most cases are diagnosed during the
first year of life. Sometimes however, the symptoms are not recognized until later in infancy or into early childhood. Secondary glaucoma occurs when another disease or eye condition causes or
contributes to increased eye pressure, resulting in optic nerve damage and vision loss.
Age is a risk factor in the development of glaucoma and this disorder can develop in anyone older than 60. However, the risk becomes apparent earlier in certain ethnic groups, such as
African-Americans, who are prone to primary open-angle glaucoma.
Race appears to be a factor, as Mexican-Americans, Asian-Americans and Japanese-Americans are also more likely to develop various types of glaucoma. For instance, acute closed-angle glaucoma is more
common among Asians. Women are at a greater risk of developing acute closed-angle glaucoma as they have shallower anterior chambers than men.
Individuals with a family history of glaucoma may be more susceptible to the disease and have a much greater risk of developing glaucoma. Primary open-angle glaucoma is three times more common in
diabetics. Other medical conditions, such as a history of high blood pressure or heart disease and hypothyroidism can increase the risk of developing glaucoma. Nearsightedness is also a risk factor.
Structural abnormalities of the eye can lead to secondary glaucoma. Injuries in the eye can result in increased eye pressure. Secondary glaucoma can be triggered after eye surgery. Prolonged use of
corticosteroid can increase the probability of developing secondary glaucoma. Glaucoma patients are advised to avoid caffeinated beverages as research has shown that a significant increase in eye
pressure can occur due to caffeine intake.
Glaucoma shows no symptoms at first but a comprehensive eye exam can detect it. A positive diagnosis of glaucoma requires the presence of elevated intraocular pressure, areas of vision loss and damage
to optic nerve.
Tonometry measures intraocular pressure (IOP) by determining the resistance of the cornea to slight indentation. Eye drops are used to numb the surface of the eye before the test. Tonometry can be
done using a puff of air, called air-puff tonometry, or using a flat-tipped cone that pushes against the corneal surface, called applanation tonometry.
An ophthalmoscope or biomicroscope allows the doctor to visualize the internal structures of the eye using a laser beam. The internal structures of the eye are depicted in the form of
three-dimensional images on a computer screen. These images can reveal any damage that may have occurred to the optic nerve or the optic disc through which the optic nerve exits the eye.
A visual field test to check for peripheral vision loss is done using a technique called tangent screen perimetry. In this technique the patient looks at a screen with an object in the center of the
screen. A second object on a wand is then moved along the sides of the patient’s visual field at a tangent to the object in the center. The ability to see the object clearly at several points along
the patient’s peripheral vision is checked.
Additional tests may be performed to arrive at an accurate diagnosis. Pachymetry may be performed to determine the thickness of the cornea which gives a measure of the intraocular pressure. Gonioscopy
may be performed to help distinguish between open-angle and closed-angle glaucoma. The drainage fluid rate may be measured using a test called tonography.
Reducing the intraocular pressure, which will prevent further damage of the optic nerve, can restrict the progress of glaucoma. However, any vision loss that may have occurred prior to treatment
cannot be reversed. Intraocular pressure can be reduced by increasing the drainage or by reducing the production of the aqueous humor, or both.
Eye drops, systemic medications, laser treatments, surgery or a combination of all these treatments can help reduce intraocular pressure. Eye drops are usually the first line of treatment for
glaucoma. There are several different types of eye drops that can be used either alone or in combination to reduce intraocular pressure.
Beta-blockers like levobunolol, timolol, carteolol, betaxolol and metipranolol reduce intraocular pressure by reducing the production of aqueous humor. Beta-blockers can cause bronchospasm and are
best avoided in patients with a history of bronchospastic disorders such as asthma and chronic obstructive pulmonary disease. These agents should also be used with caution in diabetics as they can
mask the symptoms of hypoglycemia. A reduced heart rate due to beta-blockers is a potential side effect in patients with heart disease. Beta-blocking agents are also associated with nocturnal
hypotension, a possible risk factor in the progression of glaucomatous optic nerve damage.
Alpha-adrenergic agonists like apraclonidine and brimonidine work both by decreasing aqueous humor formation and increasing drainage of aqueous humor from the eye, and require a twice-daily
administration to be effective.
Carbonic anhydrase inhibitors like dorzolamide and brinzolamide reduce the production of aqueous humor, decreasing intraocular pressure. They may require a thrice daily dosing as monotherapy, and
twice-daily dosing as adjunctive treatment. Although these drugs are slightly less effective than the beta-blockers, they are usually well tolerated. However, they can have adverse effects on patients
with hypersensitivity to sulfa drugs.
Epinephrine compounds as well as prostaglandin analogues (like latanoprost, bimatoprost and travoprost) and miotics (like pilocarpine) increase the uveoscleral outflow. These may be prescribed in
combination with drugs that reduce the production of aqueous humor. Some neuroprotective drugs that can protect the optic nerve from damage are being formulated into eye drops and are in clinical
trials for the treatment of glaucoma. These include brimonidine and memantine.
Most eye drops cause side effects like redness and itching of the eyes, headache, nausea or discoloration of skin of the eyelids. They should be used only under the advice of a medical professional
because they can interfere with the action of other drugs used for treatment of heart diseases.
Oral medications may be prescribed if eye drops fail to bring about the desired drop in intraocular pressure. Carbonic anhydrase inhibitors like acetazolamide and methazolamide are frequently
prescribed for oral use.
Surgery, referred to as a trabeculectomy operation, can be either laser guided or conventional. In this surgery an incision is made in the trabecular meshwork to allow better drainage of the aqueous
humor from the eye. In both types of surgery the eye is numbed using eye drops or by an injection of local anesthetic. The doctor then aims a laser beam at a portion of the meshwork using specialized
equipment. He may also alternately use fine surgical instruments to incise the meshwork.
Drainage implant surgery is another type of surgical procedure for treating glaucoma where the surgeon inserts a silicone tube into the eye to allow better drainage of the aqueous humor. Surgical
treatment of glaucoma may not be completely achieved with a single procedure and it may be necessary to repeat the procedure to improve the drainage.
Acute closed-angle glaucoma is a serious condition that requires immediate medical treatment. Patients should be taken to an emergency room where medications should be administered. Emergency laser
surgery called iridotomy is usually performed to prevent blindness. In this procedure a laser beam is used to cut a hole in the iris to drain the excess aqueous humor and gain quicker access to the
trabecular meshwork.
The only way to prevent the progress of glaucoma is regular eye checks, particularly after the age of 40. Regular eye exams every two to four years between the ages of 40 and 60, and every one or two
years after the age of 60 years can improve the chances of detecting glaucoma at an early stage when it can be managed with medications, and the risk of vision loss or blindness can be significantly
reduced.
Regular and correct use of medications as instructed by the doctor will ensure that the intraocular pressure does not increase to levels that could possibly damage the optic nerve.
Eating a well balanced, healthy diet that is rich in vegetables and fruits (which supply eye-friendly vitamins like vitamins A, C, E and minerals like zinc and copper) can go a long way in maintaining
eye health. It may be advisable to limit any fluid consumption to less than a quart at a time, as this could increase the intraocular pressure. Drinking small amounts of fluid at frequent intervals
throughout the day and reducing caffeine intake can also be beneficial.
Isokinetic exercises reduce intraocular pressure considerably and may be helpful in glaucoma. Brisk walking and other aerobic activity that raise the pulse just 20-25% can lower intraocular pressure
by improving blood flow to the retina and optic nerve. Rigorous exercises however, could increase intraocular pressure. It is important to consult a doctor before taking up any exercise regime.
Stress can trigger an attack of acute closed-angle glaucoma. Learning relaxation techniques to deal with stress could be useful.
Wearing protective eyewear can help prevent damage or inflammation of the eye that could lead to an increase in intraocular pressure.